Dr. Roy Stratton: From flow line to project management: Does TOC offer a unifying theory?
The pdf of the material used in the webinar
Read more on TOC-Lean-Six Sigma on TOCPA
Feedback and discussion
I have, for a long time, thought that TOC is generative rather than prescriptive. Dt Stratton makes a well reasoned argument for this viewpoint, connecting the influence of TOC thinking to several prescriptive tools and approaches. If you missed the webinar, make time to watch the video when it is published.
Jeffrey Schraeder
Attended the session; appreciated the context/perspective provided in considering multiple frameworks in comparison to TOC’s basic principles.
Joe Magid
Sindre Kentsrud:
Roy, I am a TOC/Lean novice. I believe TOC and Lean can benefit my company greatly. I am trying to convince top management (which are very cost focused) to embrace these practices. So far I have been unsuccessful. Could you give some advice on how to convince them (as well as other co-workers), and how to integrate TOC/Lean culture into a company in the best possible way? Kind regards, Sindre, Norway.
Roy’s response:
Dear Sindre,
You are not on your own but lean tends to be more readily accepted than TOC. However, when lean is accepted its is often only in part and understanding the importance of capacity buffering is often ignored resulting in only short term adoption having picked the low hanging fruit.
However, this is even more difficult in MTO and ETO environments. The question should not be which approach but the need to adopt a systems approach that uses flow as a proxy for productivity as in the Theory of Swift and even flow.
I hope my presentation shed some light on the underlying similarities between these developments and particularly lean and TOC. Any text book on operations typically presents these developments (strategy, Quality management, lean) as separate chapters – they need to be more effectively linked. TOC provides a means of doing this and clarifying the tension between local and global as well as means of resolving it. In each case (QM, lean and TOC) ongoing improvement involves the adoption of management signaling tools suited to the environment.
As a starter I would suggest you look for evidence of the dysfunctional influence of local cost and efficiency measures in building a case for change before exploring what a systems approach looks like. TOC has thinking process tools and exercises to help explore the issues and the options that do not need to be labeled so avoiding the barriers this often creates.
I hope that is of some use to you.
Roy
Ian Heptinstal:
Hi Roy. A thought on buffers and colours, what do you think? It seems to me that yellow = within control limits (common cause), but BOTH red and green are outliers and special causes. Sure red has a short-term priority over green, but for POOGI, both red and green be investigated. Implication is that “yellow = OK/expected”, and not green.
Roy’s response:
Hi Ian,
Good point. In DBR green is often seen as redundant and can be viewed as the lower control limit that might signal a change that needs to be taken note of.
In MTA yellow is more clearly the common cause region and green and red the specials requiring intervention to adjust the target.
There are limits to these comparisons as these different tools are pragmatic solutions that have proved to provide useful guidance as to when and how to intervene to meet the needs of different environments. What interests me is how some applications of lean and also TOC seam to ignore the need for such tools and particularly the continual improvement function.
Thanks for your question.
Roy
Oded Cohen’s comment:
The buffer status is a major signaling mechanism.
We are in agreement that a yellow status is a signal to management that the system is under control.
When dealing with Red and Green the signals have to be interpreted within their context.
It is important to be clear on what is the buffer monitoring and the timing of the sampling of the buffer status.
For example – in DBR and S-DBR:
- Having Green during the flow of the WO through production is not redundant. It just signals to management not to waste their valuable capacity on WOs which are flowing OK.
- Finishing a WO in green may signal that the PB may be too long. Yet, if other WOs are late or demand significant management intervention to complete on time – Green may point management in the direction that needs further improvement especially if the reason for the green is lack of proper subordination to the plan.
Regarding the Red signals:
- Reds during the flow of the WO or project – prompt management to check the situation and take recovery actions only when needed. The priority is for the checking.
- Completing a WO or a project in Red does not mean that further actions have to be taken as long as the promises for delivery and availability have been fulfilled.
Viewing TOC in a wider operations context
Loading...
ТОС, Lean and Six Sigma
Loading...
Chapter 5. Hans Steenpoorte and Michel Stijlen. Project management in a hospital: From chaos to success
From Oded Cohen and Jelena Fedurko
We are continuing to publish a new book Theory of Constrains in Practice from the TOC Strategic Solutions Library. It is a collection of cases and articles by TOC experts and practitioners from all around the world sharing their knowledge and experience gained in TOC implementations.
http://www.toc-strategicsolutions.com/en ![]()
Maasstad Hospital in Rotterdam, The Netherland, doubled the number of successfully completed projects in half the time using Critical Chain Project Management (CCPM)
Authors: Hans Steenpoorte & Michel Stijlen, Project leaders, TOC Resultants, The Netherlands
Hans Steenpoorte – The Netherlands
TOC implementer in service organizations, government, professional services, IT and healthcare. In 2006 completed Goldratt Schools Application Expert Program. Co-founder of Critical Task Manager (CTM) – TOC-based software for service organizations.
h.steenpoorte@toc-resultants.com
 Michel Stijlen – The Netherlands
Michel Stijlen – The Netherlands
TOC implementer in service organizations, government, professional services, IT and healthcare. Co-founder of Critical Task Manager (CTM) – TOC-based software for service organizations.
The article was written in October 2010
At Maasstad Hospital in Rotterdam many projects were running at the same time. Projects that were necessary to realize the ambitions of the hospital. The problem was that too many projects yielded too little result too late. Maasstad Hospital implemented Critical Chain Project Management (CCPM) and cut the average lead time in half whilst doubling the number of completed projects …… with the same number of people! Now, CCPM is an indispensable tool for innovation at the hospital.
Background
At first glance, Maasstad Hospital Rotterdam is just another hospital. In 2005, it ran into financial trouble and had to restructure completely. Since then, Maasstad Hospital has made a strong come back. It grows faster than the market and is financially healthy again. So healthy, that it confidently invested in a new hospital that it just moved into in spring 2011.
In early 2008, the recovery was in full swing and one of the problems that the management and its employees ran into was the long lead times and poor delivery performance of many projects. A survey by hospital staff led to a shocking conclusion: There were no less than one hundred eighty projects running simultaneously, and a significant number of them had no clear project leader, sponsor, scope definition, budget or due date. The Chief Innovation Officer of Maasstad Hospital explains: “Projects, and a lot of them, are inevitable for a hospital with our ambition level. But we had insufficient visibility and control over project selection, progress and completion.”
Following this sobering observation, the hospital’s board decided to invest in a project management solution that not only had to create order in the projects, but would also raise its output. They chose Critical Chain Project Management (CCPM) because it had amply proven to improve both output and due date performance of projects without increasing workload (see insert for more information about CCPM).
CCPM: Clear task priorities for outstanding project performance
Critical Chain Project Management (CCPM) was developed by Dr. Eli Goldratt, author of The Goal and Critical Chain and founder of the Theory of Constraints (TOC). CCPM is the solution for project organizations that have a low project performance in time, scope and budget.
CCPM uses the fact that project plans have more slack (“buffers”) than project teams know or want to admit: These buffers are their only means to achieve acceptable delivery performance. Or so they think …..
During project planning, CCPM takes these buffers from the task estimates and insert them in a project buffer at the end of the project. After all, it is not important for individual tasks to be completed on time, as long as the overall project is finished on time.
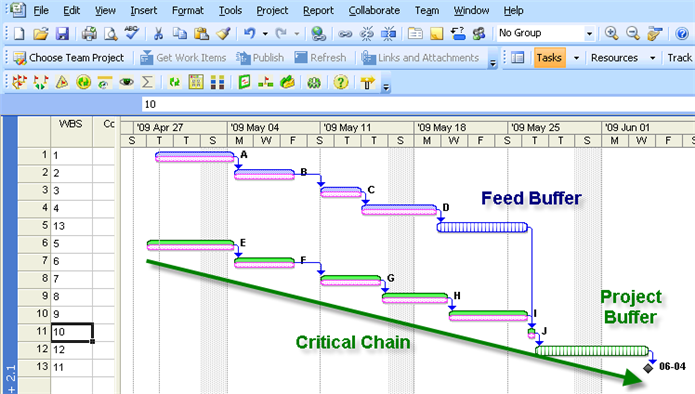
Figure 1: CCPM: The project, instead of its tasks, is protected by a time buffer
During execution, tasks that need to be executed now are regularly updated in the CCPM software by means of a remaining duration estimates: How many days till this task is completed? This estimate is then used to calculate which task consumes most of the buffer. Based on this ‘buffer consumption’ clear task priorities are calculated and depicted as green, yellow or red tasks.
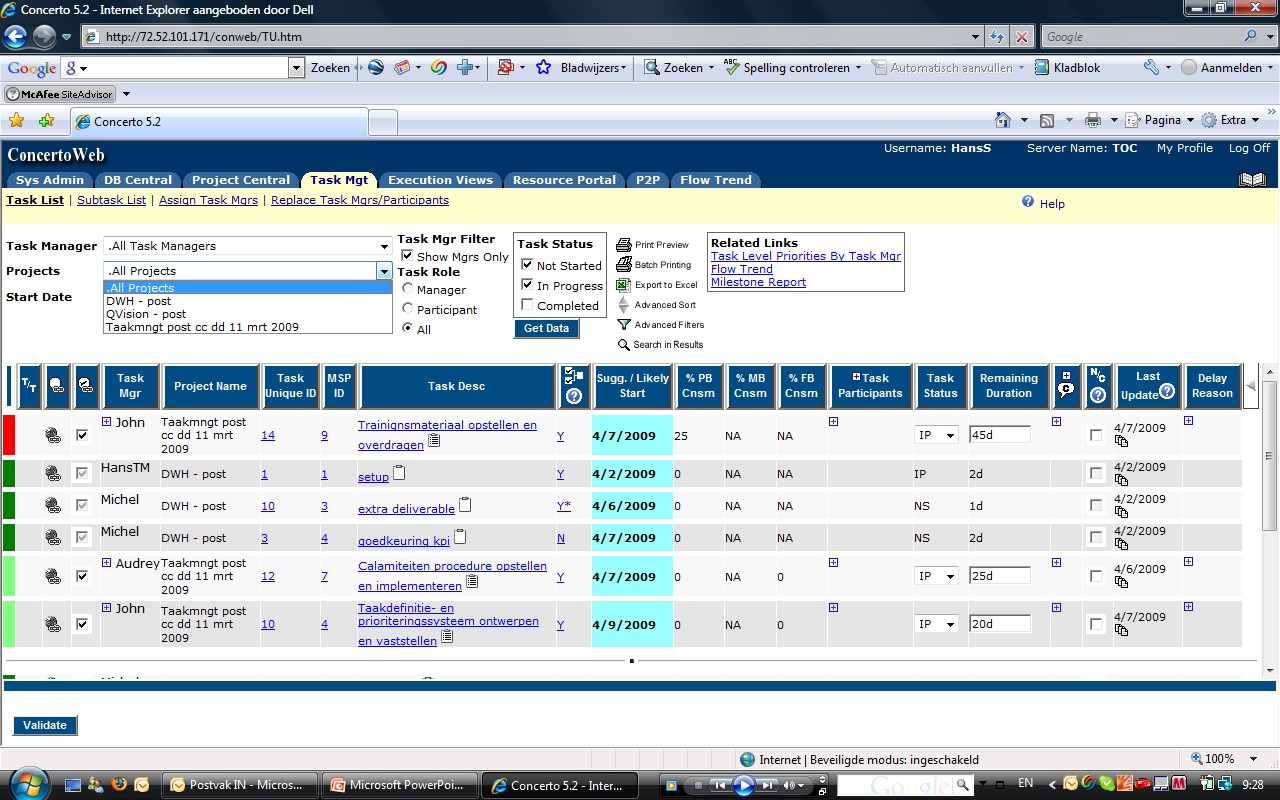
Figure 2: Colours give clear priorities within and between projects
These clear task priorities within and between projects not only end frequent discussions about project priorities, but also result in a faster and more reliable completion of projects.
Typical CCPM implementations result in the following improvements:
• Due date performance ≥ 90%
• Lead time ≈ 30% shorter
• Productivity ≈ 30% higher
• Less stress and more focus in project teams and management
CCPM has been successfully applied on a large scale in industry, IT, pharma, infrastructure & utilities. Insofar as the authors can ascertain, this application in a hospital is a first.
Yet another project
In June 2008, yet another project commenced: “Implementation of CCPM”. But the goal of this particular project was to significantly reduce the number of concurrently active projects by the end of 2009, whilst assuring that 95% of the projects are finished on time, scope (what you deliver) and budget. It was decided to focus the implementation on cross-departmental projects which caused the bulk of the load and problems at project resources in Maasstad Hospital.
To start with, the project team made an inventory of problems and discovered that they were deep rooted and fundamental:
• Some of the projects had no plan
• Some of the projects had no clear project leader or sponsor
• Projects were launched, regardless of the availability of the required staff
• Management had insufficient understanding of problems and status of active projects
• Projects were often completed too late (if a due date was set at all)
• Project group meetings were sometimes ineffective
• Projects often went over budget (if there was a formal budget)
• Project staff were not always available when needed
• There was tension and debate on priorities within and between projects
This survey also revealed that Maasstad Hospital first had to invest in basic elements of project management, in order to be ready for the implementation of CCPM.
Basic elements of project management
In a high performing project environment, every organization needs three things: structures, processes and templates.
Structures: Projects are temporary endeavours to achieve something unique. So, even more than with regular work, it is important to clearly identify roles and responsibilities. Obviously, the project leader is critical because he is responsible for the delivery of the scope (what you deliver), on time and within budget, but the sponsor also plays a key role. Each project must have a sponsor which is decisive and accessible for the project leader. The sponsor is often problem owner, provider of the necessary budget and the person who needs to approve potential deviations from the plan. Appointing decisive and accessible sponsors and assuring frequent and constructive consultation between project leader and sponsor was an important first step to success at Maasstad Hospital.
Processes: Since projects are unique, most develop, almost by definition, in a fairly unpredictable way. For this reason, it is important that key processes are in place to deal with these unforeseen developments. First, we established that projects are always in one of the following 4 phases: idea, planning, implementation and evaluation. The transition between each phase is a formal step that requires a decision by the client or the project board (see below). In order to maintain progress in active projects, brief weekly project meetings and monthly meetings with the sponsor proved critical to success.
Templates: Project management has become notorious for demanding extensive project plans that proved quite useless during execution. Hence CCPM provides plans and reports that are very concise and focused. Maasstad Hospital in Rotterdam, introduced no fewer than six templates for project ideas, project plans, project meeting notes, project status reporting, escalation, and completion reports. At first, some of these templates received some skepticism, but now they are all used extensively because they help project teams and sponsors to focus and save time.
Project Board
Besides implementing structures, processes and templates a so called Project Board was set up. The Project Board is a tightly structured meeting of the hospital’s board that included all sponsors of the cross-departmental projects. The objective of the project board is threefold: First, selection of valuable project ideas. Second, ensure effective intervention by sponsors in struggling (so called “red”) projects, and finally evaluation of completed projects.
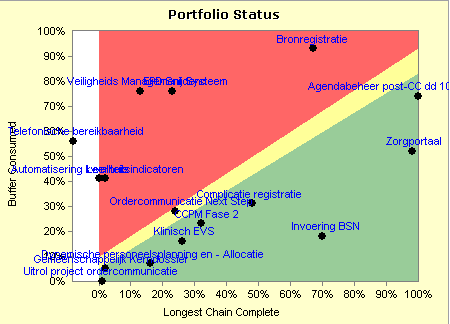
Figure 3: Transparancy about active projects and their status; green, yellow or red
At Maaststad Hospital project selection was simplified by means of a 1 page form that the author needed to discuss with a potential sponsor before proposing it to the Project Board. The Chairman of the Board then lead the discussion: “In no more than fifteen minutes, we often have five or more project ideas to discuss. I ask only three questions: Who is excited about this idea? What problem does it solve? And: What is the direction of the solution? Through question 1 and 2 we lost quite a few ideas, and normally only 1 or 2 get approved for planning, provided that at least 2 projects were completed as well. Otherwise they must wait to prevent overloading of the project resources. “
The advantage of this method is twofold. Firstly, management now is fully aware of, and committed to, all ongoing cross-departmental projects. But more importantly: During the first phase of implementation significantly less projects were started, thus reducing the work load on the scarce project resources and allowing them to focus on finishing already running projects effectively.
Besides focusing on project selection, execution and evaluation the project board also monitors the depletion of the project budget. In many organizations, projects need to be financed from departmental budgets, often leading to heated discussions at the end of the year when the overall budget appears to have been exceeded. To stop this once and for all, Maasstad Hospital took a fraction of all relevant operating budgets and inserted them into one central project budget, aimed at covering the out of pocket expenses of all cross-departmental projects. Every month, the project board monitored the real and expected exhaustion of this budget vs time using a simple report. This way the project board could monitor the budget depletion per project, but more importantly found that the inevitable budget overruns and under spends tend to offset one another provided they are financed for a single source; the cross-departmental project budget.
Finally CCPM ……
In the fall of 2008, the situation in Maasstad Hospital had significantly improved: All the projects had clear project leaders, sponsors and consensus over time (due date), scope (what they will deliver), budget (out of pocket expenses only) and goal (desired outcome). Because the project board was quite reluctant to approve new projects and even some struggling projects were stopped, the pressure on the project resources declined. It was time to introduce CCPM to further reduce lead times and increase completion.
Software can never be the aim of an improvement project, but, increasingly, it is becoming a necessary precondition. CCPM software distinguishes itself from other project management software in the sense that it is focused on execution rather than planning. After all, it is during execution that the project almost inevitably starts to deviate from the plan and more often than not, in traditional project management the plan is abandoned altogether. The solution is a robust high level plan that doesn’t detail actions, but lists deliverables, intermediate objectives necessary for achieving the project objective. Plans usually consist of no more than ten to fifteen deliverables. During execution the responsible resource can add actions to the deliverable that are deemed necessary to generate the desired outcome.
Project plans are not created by a person sitting at a computer. One of the key success factors of this CCPM implementation is the so called planning session: After approval of the project idea by the Project Board, the proposed project team gets together for a four hour meeting. In a closely facilitated meeting they go through the key elements of the project plan template in such a way, that the draft plan is filled in and ready to be sent to the sponsor for approval by the end of the meeting. At Maasstad Hospital projects are no longer started without such a planning session. In very little time it generates a focused plan with maximum buy-in that contains all elements the project team needs to execute the project successfully.
Once a project is in progress, frequent (weekly) short project team meetings are critical for success. In the weekly meetings, the project leader updates the project real time in the CCPM software, based on the input of the team members. Maasstad Hospital has even invested in a number of “CCPM-rooms” with computer and flatscreen TV’s on the wall where project teams can meet and update their project.
What is unique about this? CCPM makes very clear which project deliverables need to be worked on now and in what order of priority both and between projects. This leads to calm and focus as well as a better flow of projects. Per active deliverable, the tasks are updated by entering the estimated number of days until completion. CCPM is always forward looking: Do not spend time on what has been done, but focus on what needs to be done to finish a deliverable. And even more importantly, avoid blame if tasks were completed late. Accept windfalls and setbacks as a fact of life in a project environment and focus continually on corrective actions and decisions that lead to completion of the project on time, scope and budget.
Through the CCPM implementation, Maasstad Hospital learnt that project management is a vital but often underestimated craft. For that reason, it secured the continuation and development of CCPM knowledge in an in-house project office. The project office provides training courses for project teams and leaders, facilitates planning sessions, prepares project board meetings and gives (un)solicited assistance to projects that are in red.
Results: Doubling the output and halving the lead time
Between late 2008 and spring 2009, all the old projects were finished and new projects under CCPM principles introduced. Due to its success, the management has decided to add a group of existing projects related to the construction of the new hospital to the CCPM portfolio (see the increase in the summer of 2009 in Figure 4 below). Nevertheless, the number of cross-departmental projects that ran simultaneously in Maasstad Hospital remained fairly stable with approximately 30, versus over 40 at the start in mid 2008. This decrease is critical to the focus of project resources and the flow of projects.
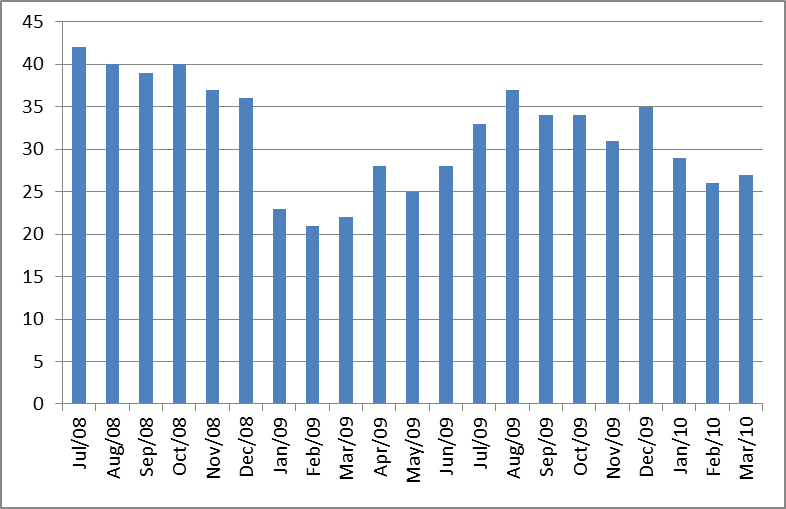
Figure 4: Number of concurrent cross-departmental projects declined from around 40 to under 30 despite growing the portfolio
The fact that Maasstad Hospital could add a significant number of projects to its portfolio was due to the fact that they finished much faster than before. Figure 5 shows that the average lead time of cross-departmental projects has decreased from over 2 years in 2008 to approximately 10 months in 2009 and 2010. This is less than half the lead time!
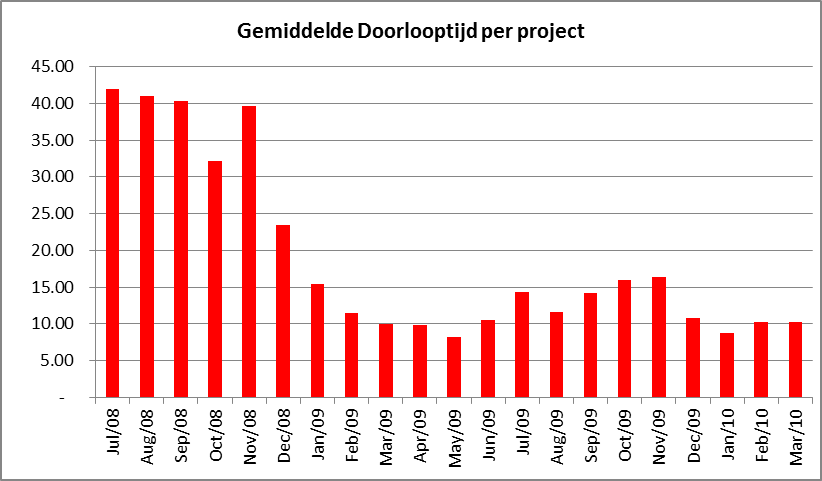
Figure 5: Average lead time (in # of months) of cross-departmental projects was cut in less than half
This brings us to the last and most important achievement: In 2008, on average 1 cross-departmental project was finished per month. The Chairman of the Board concludes: “By introducing project management principles and CCPM, the productivity of our project resources nearly tripled. Currently we finish about 3 cross-departmental projects per month. Project management has become a core competency of Maasstad Hospital towards achieving our ambition; making Rotterdam the healthiest city in the Netherlands.”
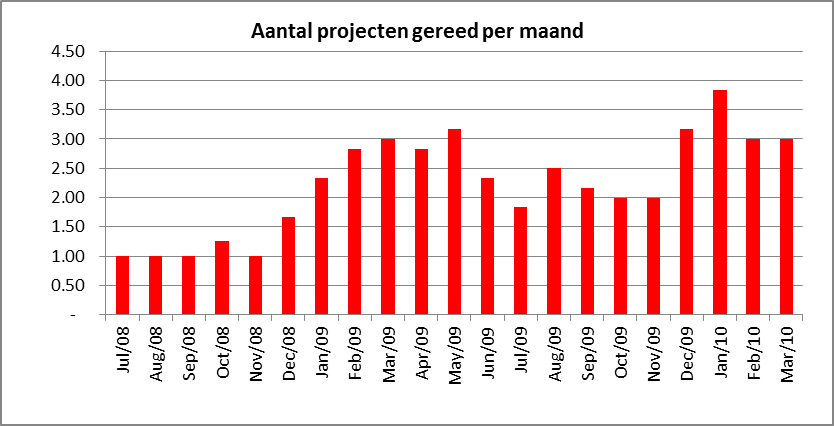
Figure 6: Number of projects finished per month tripled (6-month rolling average)
Lessons for successful implementation
Maasstad Hospital Rotterdam had too many projects that often ran late and yielded too little result. CCPM has been implemented, resulting in doubling the speed of delivery and a tripling the number of completed projects.
What is critical to achieving success?
1. Implement simple structures, processes and templates for all projects
2. Install a Project Board at board level to select projects and evaluate and monitor progress
3. Create a central budget for all out of pocket expenses and avoid planning and monitoring of internal hours
4. CCPM project management is a craft: Use an experienced implementer and retain the knowledge and skills in a project office
5. Accept windfalls and setbacks as a “fact of life” and keep project teams focused on completing projects on time, scope and budget
Learn more about project management and CCPM:
– Goldratt, Eliyahu M., Critical Chain
– Nokes, Major, Greenwood, Allen, Goodman, The Definitive Guide to Project Management, Prentice Hall- Financial Times
– www.realization.com
– www.toc-resultants.com